Ciwon Daji na Pancreatic
Ciwon daji na pancreatic Ya kasan ce yana tasowa lokacin da (cell)wato ƙwayoyin jini a cikin pancreas, sashin glandular bayan ciki, ya fara ninkawa daga sarrafawa kuma ya zama taro . Wadannan kwayoyin cutar daji suna da ikon mamaye wasu sassan jiki. [1] An san adadin nau'ikan ciwon daji na pancreatic. [2]
| Ciwon Daji na Pancreatic | |
|---|---|
 | |
| Description (en) | |
| Iri |
endocrine gland cancer (en) cuta |
| Specialty (en) |
oncology gastroenterology (en) |
| Symptoms and signs (en) |
Ciwon ciki, Shawara, acute pancreatitis (en) Trousseau's syndrome (en) |
| Physical examination (en) |
medical ultrasonography (en) positron emission tomography (en) |
| Genetic association (en) |
SBF2 (en) |
| Medical treatment (en) | |
| Magani |
octreotide (en) |
| Identifier (en) | |
| ICD-10-CM | C25.0, C25.1 da C25.2 |
| ICD-9-CM | 157.1, 157.8, 157.0 da 157.2 |
| OMIM | 260350 |
| DiseasesDB | 9510 |
| MedlinePlus | 000236 |
| eMedicine | 000236 |
| Disease Ontology ID | DOID:1793 |


Mafi na kowa, adenocarcinoma pancreatic, lissafin kusan 90% na lokuta, [3] da kalmar "ciwon daji na pancreatic" wani lokaci ana amfani da shi kawai ga irin wannan. [2] Wadannan adenocarcinomas suna farawa ne a cikin sashin pancreas wanda ke yin enzymes masu narkewa . [2] Wasu nau'o'in ciwon daji da dama, waɗanda ke wakiltar yawancin marasa adenocarcinomas, suna iya tasowa daga waɗannan kwayoyin halitta. [2] Kimanin kashi 1-2% na lokuta na ciwon daji na pancreatic ne neuroendocrine ciwace-ciwacen daji, wanda ya taso daga kwayoyin samar da hormone na pancreas. [2] Waɗannan gabaɗaya ba su da ƙarfi fiye da adenocarcinoma na pancreatic. [2]
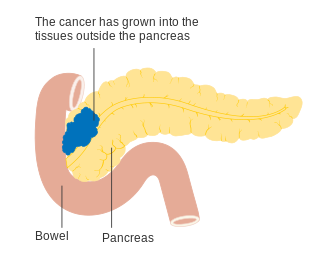
Alamu da ciwon daji na pancreatic da aka fi sani na iya haɗawa da launin rawaya fata, ciwon ciki ko baya, asarar nauyi da ba a bayyana ba, stools mai launin haske, fitsari mai duhu, da asarar ci . [4] Yawancin lokaci, ba a ganin alamun cutar a farkon matakan cutar, kuma alamun da ke da takamaiman isa don nuna ciwon daji na pancreatic yawanci ba sa tasowa har sai cutar ta kai mataki na gaba. [5][4] A lokacin ganewar asali, ciwon daji na pancreatic ya yadu zuwa wasu sassan jiki.[6][2]
Ciwon daji na pancreatic da wuya yana faruwa kafin shekaru 40, kuma fiye da rabin lokuta na adenocarcinoma na pancreatic yana faruwa a cikin waɗanda suka wuce 70. [5] Abubuwan haɗari don ciwon daji na pancreatic sun haɗa da shan taba, kiba, ciwon sukari, da wasu yanayi na kwayoyin halitta. [5] Kimanin kashi 25% na lokuta suna da alaƙa da shan taba, [7] da 5-10% suna da alaƙa da kwayoyin gado . [7] Ciwon daji na pancreatic yawanci ana gano shi ta hanyar haɗin fasahar hoto na likitanci kamar duban dan tayi ko ƙididdiga na hoto, gwajin jini, da gwajin samfuran nama ( biopsy ). [7][8] An rarraba cutar zuwa matakai, daga farkon (mataki I) zuwa marigayi (mataki IV).[6] Ba a sami nasarar tantance yawan jama'a ba. [9]
Haɗarin kamuwa da ciwon daji na pancreatic yana da ƙasa a tsakanin masu shan taba, da mutanen da ke kula da lafiyayyen nauyi kuma suna iyakance cin su na ja ko nama da aka sarrafa . [10] Damar masu shan taba na kamuwa da cutar suna raguwa idan sun daina shan taba kuma kusan komawa zuwa na sauran jama'a bayan shekaru 20. shekaru. [2] Ana iya magance ciwon daji na pancreatic tare da tiyata, radiotherapy, chemotherapy, palliative care, ko haɗuwa da waɗannan. [4] Zaɓuɓɓukan magani sun dogara ne akan matakin ciwon daji. [4] Tiyata ita ce kawai magani wanda zai iya warkar da adenocarcinoma na pancreatic, [6] kuma ana iya yin shi don inganta yanayin rayuwa ba tare da yuwuwar warkewa ba.[4][6] Gudanar da ciwo da magunguna don inganta narkewa ana buƙatar wasu lokuta. [6] Ana ba da shawarar kula da jin daɗi da wuri har ma ga waɗanda ke karɓar magani da ke nufin magani.[11]
A cikin 2015, ciwon daji na pancreatic kowane iri ya haifar da mutuwar 411,600 a duniya. [12] Ciwon daji na pancreatic shine sanadin mutuwa na biyar-mafi yawan gama gari daga cutar kansa a Burtaniya, [13] kuma na uku mafi yawan jama'a a Amurka. [14] Cutar ta fi faruwa a kasashen da suka ci gaba, inda kusan kashi 70% na sabbin cututtukan da aka samu a shekarar 2012 suka samo asali. [2] Pancreatic adenocarcinoma yawanci yana da mummunan tsinkaya; Bayan ganewar asali, 25% na mutane suna rayuwa shekara guda kuma 5% suna rayuwa har tsawon shekaru biyar. [2] [15] Ga cututtukan daji da aka gano da wuri, adadin rayuwa na shekaru biyar ya tashi zuwa kusan 20%. [16] Ciwon daji na Neuroendocrine yana da sakamako mafi kyau; na biyar shekaru daga ganewar asali, 65% na wadanda aka gano suna rayuwa, ko da yake rayuwa ta bambanta da yawa dangane da nau'in ciwon daji. [3]
Nau'ukan
gyara sashe
Yawancin nau'ikan ciwon daji na pancreatic ana iya raba su zuwa ƙungiyoyin gaba ɗaya. Mafi yawan lokuta (kimanin 95%) suna faruwa a cikin sashin pancreas wanda ke samar da enzymes masu narkewa, wanda aka sani da bangaren exocrine . An bayyana nau'ikan nau'ikan nau'ikan nau'ikan cututtukan ƙwayar cuta na exocrine na pancreatic, amma ganewar asali da magani suna da yawa a gama gari. Ƙananan ƙananan ciwon daji da ke tasowa a cikin samar da hormone ( endocrine ) na pancreas suna da halaye daban-daban na asibiti kuma ana kiran su ciwon daji na neuroendocrine na pancreatic, wani lokacin an rage su a matsayin "PanNETs". Dukansu ƙungiyoyin biyu suna faruwa ne musamman (amma ba na musamman) a cikin mutane sama da 40 ba, kuma sun ɗan fi yawa a cikin maza, amma wasu nau'ikan nau'ikan da ba a cika samun su ba galibi suna faruwa a cikin mata ko yara.[17][18]
Exocrine cancers
gyara sasheƘungiyar exocrine ta mamaye adenocarcinoma na pancreatic (saɓanin wannan suna na iya ƙara "masu cin zarafi" da "ductal"), wanda shine mafi yawan nau'i na yau da kullum, wanda ke wakiltar kimanin kashi 85 cikin dari na dukan ciwon daji na pancreatic.[5] Kusan duk waɗannan suna farawa a cikin bututun pancreas, azaman pancreatic ductal adenocarcinoma (PDAC). [19] Wannan shi ne duk da cewa nama daga abin da ya taso - na pancreatic ductal epithelium - wakiltar kasa da 10% na pancreas ta hanyar girma cell, domin shi ya ƙunshi kawai ducts (wani m amma capillary-kamar duct-tsarin fanko) a ciki. pancreas. [20] Wannan ciwon daji ya samo asali ne a cikin bututun da ke ɗauke da ɓoye (kamar enzymes da bicarbonate ) daga pancreas. Kimanin kashi 60-70% na adenocarcinomas suna faruwa a cikin kan pancreas . [5]
Nau'in na gaba-mafi yawan gaske, acinar cell carcinoma na pancreas, yana tasowa a cikin gungu na sel waɗanda ke samar da waɗannan enzymes, kuma suna wakiltar 5% na ciwon daji na exocrine na pancreas. Kamar wadanda aka bayyana 'ayyukan ensincrrrrrer a kasa, Carcinomas Carcinomas da aka bayyana a ƙasa, Carjin Carcinomas ya bayyana a kasa, Carcinoman Carcinomas na iya haifar da samar da wasu kwayoyin, a wannan yanayin narkar da enzymes, wanda zai haifar da bayyanar da enzymes, wanda zai haifar da bayyanar cututtuka kamar jin zafi.
Cystadenocarcinomas yana da kashi 1% na ciwon daji na pancreatic, kuma suna da kyakkyawan hangen nesa fiye da sauran nau'in exocrine. [21]
Pancreatoblastoma wani nau'i ne da ba kasafai ba, galibi yana faruwa a lokacin ƙuruciya, kuma yana da kyakkyawan hasashen. Sauran cututtukan cututtuka na exocrine sun haɗa da carcinomas adenosquamous, carcinomas cell carcinomas, carcinomas hepatoid carcinomas, colloid carcinomas, carcinomas marasa bambanci, da carcinomas marasa daidaituwa tare da osteoclast -like giant sel . M ciwon daji na pseudopapillary wani ƙananan ƙananan neoplasm ne wanda ke shafar ƙananan mata, kuma gabaɗaya yana da tsinkaye mai kyau.[5][21][20]
Pancreatic mucinous cystic neoplasms babban rukuni ne na ciwace-ciwacen ƙwayar cuta wanda ke da bambance-bambancen m. Ana gano su da haɓaka sosai yayin da CT scans ke ƙara ƙarfi da gama gari, kuma ana ci gaba da tattaunawa kan yadda za a iya tantance su da kuma bi da su, ganin cewa da yawa ba su da kyau. [22]
Neuroendocrine
gyara sasheƘananan ciwace-ciwacen da ke tasowa a wasu wurare a cikin pancreas sune ciwace-ciwacen ƙwayoyin cuta na neuroendocrine (PanNETs). [23] Ciwon daji na Neuroendocrine (NETs), ya kasan ce su ne nau'i-nau'in daban-daban na ciwon daji ko ciwon daji wanda ke tasowa daga kwayoyin neuroendocrine na jiki, wanda ke da alhakin haɗakar da tsarin juyayi da endocrin. NETs na iya farawa a yawancin gabobin jiki, gami da pancreas, inda nau'ikan mugayen nau'ikan duka ana ɗaukar su ba kasafai bane . PanNETs an haɗa su zuwa nau'ikan 'aiki' da 'marasa aiki', ya danganta da matakin da suke samar da hormones. Nau'in aiki suna ɓoye hormones kamar insulin, gastrin, da glucagon a cikin jini, sau da yawa a cikin adadi mai yawa, suna haifar da alamun bayyanar cututtuka kamar ƙarancin sukari na jini, amma kuma suna fifita ganowa da wuri. Mafi yawan aiki PanNETs sune insulinomas da gastrinomas, mai suna bayan hormones da suke ɓoyewa. Nau'in da ba sa aiki ba sa ɓoye hormones da yawa don haifar da bayyanar cututtuka na asibiti, don haka PanNETs marasa aiki ana gano su ne kawai bayan ciwon daji ya yadu zuwa wasu sassan jiki. [24]
Kamar yadda yake tare da sauran ciwace-ciwacen neuroendocrine, tarihin kalmomi da rarrabuwa na PanNETs yana da rikitarwa.[23] A wasu lokuta ana kiran PanNETs "cututtukan ƙwayoyin tsibiri", [25] ko da yake yanzu an san su ba su tashi daga ƙwayoyin tsibiri kamar yadda ake tunani a baya ba. [24]
Alamomi da alamomi
gyara sashe
Tunda ciwon daji na pancreatic yawanci ba ya haifar da alamun da za a iya gane su a farkon matakansa, yawanci ba a gano cutar ba har sai ta yadu fiye da pancreas kanta.[8] Wannan yana ɗaya daga cikin manyan dalilan rashin ƙarancin rayuwa gabaɗaya. Banda wannan shine PanNETs masu aiki, inda yawan samar da hormones masu aiki daban-daban na iya haifar da bayyanar cututtuka (wanda ya dogara da nau'in hormone).[26]
Da yake la'akari da cewa ba kasafai ake gano cutar ba kafin shekaru 40, alamomin alamun adenocarcinoma na pancreatic da ke faruwa kafin a gano cutar sun haɗa da:
- Ciwo a cikin babba ko baya, yawanci yaduwa daga kewayen ciki zuwa baya. Wurin da ke ciwo zai iya nuna ɓangaren ƙwayar ƙwayar ƙwayar ƙwayar ƙwayar ƙwayar cuta. Zafin na iya zama mafi muni da dare kuma yana iya karuwa akan lokaci don ya zama mai tsanani kuma maras ƙarewa.[27] Ana iya samun sauƙi kaɗan ta hanyar lankwasawa. A Burtaniya, kusan rabin sabbin cututtukan daji na pancreatic ana gano su ne bayan ziyartar sashen gaggawa na asibiti don jin zafi ko jaundice. A cikin kashi biyu bisa uku na mutane, ciwon ciki shine babban alama, don 46% na jimlar tare da jaundice, tare da 13% suna da jaundice ba tare da jin zafi ba.[6]
- Jaundice, launin rawaya mai launin rawaya zuwa fararen idanu ko fata, tare da ko ba tare da jin zafi ba, kuma mai yiwuwa a hade tare da fitsari mai duhu, yana haifar da lokacin da ciwon daji a cikin kan pancreas ya toshe ƙwayar bile na kowa yayin da yake tafiya ta cikin pancreas. [28]
- Rage nauyi wanda ba a bayyana ba, ko dai daga asarar ci, ko asarar aikin exocrine wanda ke haifar da rashin narkewa . [6]
- Ciwon daji na iya damfara sassan da ke makwabtaka da su, yana rushe hanyoyin narkewar abinci da kuma sanya shi da wahala ga ciki ya zama fanko, wanda zai iya haifar da tashin zuciya da jin cikawa. Kitsen da ba a narkar da shi ba yana kaiwa ga ƙamshi mai ƙamshi, ƙashin ƙazanta waɗanda ke da wuyar gushewa.[6] Maƙarƙashiya kuma yana da yawa. [29]
- Aƙalla 50% na mutanen da ke da adenocarcinoma pancreatic suna da ciwon sukari a lokacin ganewar asali.[5] Yayin da ciwon sukari mai tsayi ya kasance sanannen haɗari ga ciwon daji na pancreatic (duba abubuwan haɗari ), ciwon daji zai iya haifar da ciwon sukari, wanda a cikin yanayin kwanan nan na ciwon sukari za a iya la'akari da farkon alamar cutar. [30] Mutanen sama da 50 waɗanda ke haɓaka ciwon sukari suna da haɗarin haɓaka adenocarcinoma na pancreatic sau takwas a cikin shekaru uku, bayan haka haɗarin dangi ya ragu.[6]
Sauran binciken
gyara sashe- Ciwon daji na Trousseau - wanda zubar da jini ya haifar da sauri a cikin tasoshin jini na portal ( portal vein thrombosis ), zurfin veins na extremities ( deep vein thrombosis ), ko kuma na sama ( na waje thrombosis ) a ko'ina a cikin jiki - na iya hade da shi. ciwon daji na pancreatic, kuma ana samunsa a kusan kashi 10% na lokuta. [7]
- An ba da rahoton baƙin ciki na asibiti tare da haɗin gwiwa tare da ciwon daji na pancreatic a cikin wasu 10-20% na lokuta, kuma yana iya zama cikas ga kulawa mafi kyau. Bacin rai wani lokaci yana bayyana kafin a gano cutar kansa, yana nuna cewa ilimin halittar cutar na iya kawo shi. [7]
Sauran bayyanar cututtuka na yau da kullum sun hada da rauni da gajiyawa sauƙi, bushe baki, matsalolin barci, da ƙwayar ciki mai laushi . [29]
Alamomin yaduwa
gyara sashe
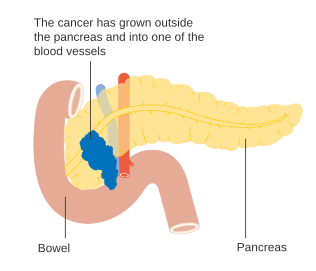
Yaduwar ciwon daji na pancreatic zuwa wasu gabobin ( metastasis ) na iya haifar da bayyanar cututtuka. Yawanci, adenocarcinoma na pancreatic na farko yana yaduwa zuwa nodes na lymph na kusa, kuma daga baya zuwa hanta ko zuwa ga kogin peritoneal, babban hanji, ko huhu.[7] Ba kasafai ba, yana yaduwa zuwa kashi ko kwakwalwa. [31]
Ciwon daji a cikin pancreas kuma yana iya zama ciwon daji na biyu da ya yadu daga wasu sassan jiki. Wannan ba sabon abu ba ne, ana samun shi a kusan kashi 2% na lokuta na ciwon daji na pancreatic. Ciwon daji na koda shine mafi yawan ciwon daji da ke yaduwa zuwa ga pancreas, sannan kuma ciwon daji na launin fata, sannan kuma ciwon daji na fata, nono, da huhu . Ana iya yin tiyata a kan maƙarƙashiya a irin waɗannan lokuta, ko da begen magani ko don rage alamun. [32]
Abubuwan haɗari
gyara sasheAbubuwan haɗari ga adenocarcinoma na pancreatic sun haɗa da:[5][2][6][33][34]
- Shekaru, jima'i, da kabilanci - haɗarin tasowa ciwon daji na pancreatic yana ƙaruwa da shekaru. Yawancin lokuta suna faruwa bayan shekaru 65,[2] yayin da lokuta kafin shekaru 40 ba a saba gani ba. Cutar ta fi yawa a cikin maza fiye da mata. [2] A Amurka, ya fi fiye da sau 1.5 a cikin Baƙin Amurkawa, ko da yake faruwa a Afirka ba shi da yawa. [2]
- Shan taba sigari ita ce mafi kyawun abin da za a iya kauce masa don kamuwa da ciwon daji na pancreatic, kusan haɗarin ninki biyu tsakanin masu shan taba na dogon lokaci, haɗarin yana ƙaruwa tare da adadin shan taba da kuma shekarun shan taba. Hadarin yana raguwa sannu a hankali bayan daina shan taba, yana ɗaukar shekaru 20 don komawa kusan na marasa shan taba. [35]
- Kiba - ma'aunin jiki fiye da 35 yana ƙara haɗarin dangi da kusan rabin.[6][36]
- Tarihin iyali - 5-10% na ciwon daji na pancreatic yana da wani bangare na gado, inda mutane ke da tarihin iyali na ciwon daji na pancreatic.[5][37] Haɗarin yana ƙaruwa sosai idan dangi fiye da ɗaya na farko sun kamu da cutar, kuma mafi ƙanƙanta idan sun kamu da ita kafin shekaru 50.[8] Yawancin kwayoyin halittar da ke tattare da su ba a gano su ba.[5][38] Gadon pancreatic na gada yana ba da ƙarin haɗarin rayuwa na ciwon daji na pancreatic na 30-40% zuwa shekaru 70. [7] Ana iya ba da gwajin cutar sankara na pancreatic ga mutanen da ke da gadaje na pancreatitis bisa tushen bincike.[39] Wasu mutane na iya zaɓar a cire musu ƙwayar ƙwayar cuta ta hanyar tiyata don hana ciwon daji daga tasowa a nan gaba. [7]
- An haɗu da ciwon daji na pancreatic tare da waɗannan nau'o'in cututtuka na gado: Peutz-Jeghers ciwo saboda maye gurbi a cikin ƙwayar cuta ta STK11 (mai wuyar gaske, amma mai haɗari mai karfi); dysplastic nevus ciwo (ko iyali atypical mahara tawadar Allah da melanoma ciwo, FAMMM-PC) saboda maye gurbi a cikin CDKN2A tumor suppressor gene; autosomal recessive ataxia-telangiectasia da autosomal maye gurbi a cikin kwayoyin BRCA2 da PALB2 ; ciwon daji marasa polyposis na gado (Lynch syndrome); da kuma iyali adenomatous polyposis . PanNETs an haɗa su da nau'in neoplasia na endocrine da yawa (MEN1) da von Hippel Lindau ciwo.[7][5][8]
- Pancreatitis na yau da kullun yana bayyana kusan haɗarin sau uku, kuma kamar yadda yake tare da ciwon sukari, sabon ciwon pancreatitis na iya zama alamar ƙari.[7] Hadarin ciwon daji na pancreatic a cikin mutanen da ke da dangi na pancreatic yana da girma musamman. [7][38]
- Ciwon sukari mellitus abu ne mai haɗari ga ciwon daji na pancreatic kuma (kamar yadda aka gani a cikin sashin Alamu da alamomi ) sabon ciwon sukari na iya zama alamar farkon cutar. Mutanen da aka gano suna da nau'in ciwon sukari na 2 na tsawon fiye da shekaru 10 na iya samun haɗarin 50%, idan aka kwatanta da mutanen da ba su da ciwon sukari.[7] A cikin 2021, Venturi ya ba da rahoton cewa pancreas yana iya ɗaukar cesium mai yawa na rediyoaktif (Cs-134 da Cs-137) yana haifar da pancreatitis na yau da kullun kuma mai yiwuwa kansar pancreatic tare da lalata tsibiran pancreatic, yana haifar da nau'in ciwon sukari na 3c (pancreatogenic) . [40] Pancreatic na yau da kullun, ciwon daji na pancreatic da ciwon sukari mellitus sun ƙaru a cikin gurɓataccen yawan jama'a, musamman yara da matasa, bayan abubuwan nukiliyar Fukushima da Chernobyl. A lokaci guda, cututtuka na pancreatic a duniya, ciwon sukari da radiocesium na muhalli suna karuwa.
- Ba a nuna takamaiman nau'ikan abinci (kamar yadda ya bambanta da kiba) a fili don ƙara haɗarin ciwon daji na pancreatic.[5][41] Abubuwan da ake ci waɗanda wasu shaidu ke nuna ɗan ƙaramin haɗari sun haɗa da nama da aka sarrafa, jan nama, da naman da aka dafa a yanayin zafi sosai (misali ta soya, broiling, ko gasa). [41][42]
Barasa
gyara sasheShan barasa fiye da kima shine babban abin da ke haifar da cutar sankarau na yau da kullun, wanda hakan ke haifar da ciwon daji na pancreatic, amma babban bincike ya kasa tabbatar da shan barasa a matsayin abin haɗari kai tsaye ga kansar pancreatic. Gabaɗaya, ƙungiyar tana da rauni akai-akai kuma yawancin binciken ba su sami wata ƙungiya ba, tare da shan taba mai ƙarfi mai ruɗani . Shaidar ta fi ƙarfi don haɗin gwiwa tare da sha mai yawa, na aƙalla sha shida a kowace rana.[7][43]
Pathophysiology
gyara sashe_Case_01.jpg)
Ciwon daji
gyara sashe
Ana tsammanin ciwon daji na exocrine yana tasowa daga nau'o'in ciwon daji da yawa a cikin pancreas, amma waɗannan raunuka ba koyaushe suna ci gaba zuwa ciwon daji ba, kuma yawan adadin da aka gano a matsayin sakamakon karuwar amfani da CT scans don wasu dalilai ba a magance su ba.[7] Baya ga pancreatic serous cystadenomas, wanda kusan kullum ba su da kyau, ana gane nau'in ciwon daji guda hudu.
Na farko shi ne pancreatic intraepithelial neoplasia . Waɗannan raunukan ƙananan ƙwayoyin cuta ne a cikin pancreas kuma galibi ana samun su a cikin gawawwakin mutanen da ba su da cutar kansa. Wadannan raunuka na iya ci gaba daga ƙananan zuwa babban matsayi sannan zuwa ƙari. Fiye da kashi 90% na shari'o'i a duk maki suna ɗauke da kwayar halittar KRAS mara kyau, yayin da suke cikin maki. 2 da 3, lalacewar wasu kwayoyin halitta guda uku - CDKN2A ( p16 ), p53, da SMAD4 – ana ƙara samun sau da yawa.[5]
Nau'i na biyu shine intraductal papillary mucinous neoplasm (IPMN). Waɗannan raunuka ne na macroscopic, waɗanda ake samu a kusan kashi 2% na duk manya. Wannan adadin yana ƙaruwa zuwa kusan 10% ta shekaru 70. Waɗannan raunukan suna da kusan kashi 25% na haɗarin haɓakawa zuwa cutar kansa. Suna iya samun maye gurbin halittar KRAS (40-65% na lokuta) kuma a cikin GNAS Gs alpha subunit da RNF43, suna shafar hanyar siginar Wnt .[5] Ko da an cire su ta hanyar tiyata, ƙarin haɗarin da ke tattare da ciwon daji na pancreatic yana tasowa daga baya.[7]
Nau'i na uku, pancreatic mucinous cystic neoplasm (MCN), galibi yana faruwa a cikin mata, kuma yana iya kasancewa mara kyau ko kuma ci gaba zuwa kansa. [44] Idan waɗannan raunuka sun zama manya, suna haifar da alamun bayyanar cututtuka, ko kuma suna da siffofi masu ban sha'awa, yawanci ana iya samun nasarar cire su ta hanyar tiyata.[7]
Nau'i na huɗu na ciwon daji da ke tasowa a cikin pancreas shine intraductal tubulopapillary neoplasm. Wannan nau'in WHO ta gane shi a cikin 2010 kuma ya ƙunshi kusan kashi 1-3% na dukkanin neoplasms na pancreatic. Matsakaicin shekarun da aka gano shine shekaru 61 (shekaru 35-78). Kusan kashi 50 cikin 100 na waɗannan raunuka sun zama masu mamayewa. Bincike ya dogara da ilimin tarihi, saboda waɗannan raunuka suna da wuyar bambanta da sauran raunuka a kan ko dai na asibiti ko na rediyo. [45]
Ciwon daji mai cutarwa
gyara sasheAbubuwan da suka faru na kwayoyin halitta da aka samo a cikin ductal adenocarcinoma an yi su da kyau, kuma an yi cikakken jerin abubuwan da suka faru don nau'in ciwon daji na kowa. Kwayoyin halitta guda hudu an gano kowannensu an canza su a yawancin adenocarcinomas: KRAS (a cikin 95% na lokuta), CDKN2A (kuma a cikin 95%), TP53 (75%), da SMAD4 (55%). Na ƙarshe daga cikin waɗannan yana da alaƙa musamman tare da tsinkaye mara kyau. [7] SWI/SNF maye gurbi/ shafewa yana faruwa a cikin kusan 10-15% na adenocarcinomas.[5] An kuma yi bincike kan sauye-sauyen kwayoyin halitta a wasu nau'ikan ciwon daji na pancreatic da raunukan da suka rigaya ya faru. [7] Binciken fassarar fassarar da jerin mRNA don nau'ikan ciwon daji na pancreatic na gama gari sun gano cewa kashi 75% na kwayoyin halittar ɗan adam ana bayyana su a cikin ciwace-ciwacen ciwace-ciwacen daji, tare da wasu kwayoyin halittar 200 waɗanda aka fi bayyana su musamman a cikin ciwon daji na pancreatic idan aka kwatanta da sauran nau'ikan ƙari.[46][47]
PanNETs
gyara sasheKwayoyin halittar da ake samu sau da yawa a cikin PanNETs sun bambanta da waɗanda ke cikin ciwon daji na pancreatic exocrine. [48] Misali, maye gurbin KRAS yawanci baya nan. Maimakon haka, maye gurbi na MEN1 na gado yana haifar da ciwo na MEN1, wanda ciwace-ciwacen farko ke faruwa a cikin glandon endocrin guda biyu ko fiye. Kimanin kashi 40-70% na mutanen da aka haifa tare da maye gurbi na MEN1 a ƙarshe suna haɓaka PanNet. [49] Sauran kwayoyin halittar da ake yawan canzawa sun hada da DAXX, mTOR, da ATRX .[24]
Bincike
gyara sashe

Alamun adenocarcinoma na pancreatic ba ya kan bayyana a farkon cutar, kuma ba su bambanta da cutar ba. Alamun da ake gano cutar sun bambanta bisa ga wurin da ciwon daji yake a cikin pancreas, wanda masana ilimin halittar jiki suka raba (daga hagu zuwa dama akan mafi yawan zane) zuwa kai mai kauri, wuyansa, da jikin da ke tafe, yana ƙarewa a cikin wutsiya.
Ba tare da la'akari da wurin da ƙari yake ba, alamar da aka fi sani da ita ita ce asarar nauyi da ba a bayyana ba, wanda zai iya zama babba. Yawancin 'yan tsiraru (tsakanin kashi 35 zuwa 47%) na mutanen da aka gano suna da cutar za su sami tashin zuciya, amai, ko jin rauni. Ciwon daji a cikin kan pancreas yawanci kuma yana haifar da jaundice, zafi, asarar ci, fitsari mai duhu, da stools masu launin haske. Ciwon daji a jiki da wutsiya yakan haifar da ciwo.
Wasu lokuta mutane suna samun farkon farkon ciwon sukari na 2 wanda ke da wuyar sarrafawa, tarihin kwanan nan amma ba a bayyana kumburin jini ba wanda ya haifar da ɗigon jini ( thrombophlebitis ) wanda aka fi sani da alamar Trousseau, ko kuma wani harin da ya gabata na pancreatitis . Likita na iya zargin ciwon daji na pancreatic lokacin da farkon ciwon sukari a cikin wanda ya haura shekaru 50 yana tare da alamu na yau da kullun kamar asarar nauyi da ba a bayyana ba, ci gaba na ciki ko baya, rashin narkewar abinci, amai, ko najasa mai kitse. Jaundice tare da kumburin gallbladder mara raɗaɗi (wanda aka sani da alamar Courvoisier ) na iya haifar da zato, kuma yana iya taimakawa wajen bambanta ciwon daji na pancreatic da gallstones .
Ana amfani da dabarun daukar hoto na likitanci, irin su na'urar daukar hoto (CT scan) da endoscopic duban dan tayi (EUS) duka don tabbatar da ganewar asali da kuma taimakawa wajen yanke shawara ko za'a iya cire ƙwayar cutar ta hanyar tiyata (" sabuntawa "). A sabanin CT scan, ciwon daji na pancreatic yawanci yana nuna karuwa a hankali a hankali radiyo, maimakon wankewa da sauri kamar yadda ake gani a cikin ƙwayar cuta ta al'ada ko jinkirin wankewa kamar yadda ake gani a cikin pancreatitis na kullum. Hakanan za'a iya amfani da Hoto na Magnetic Resonance Hoto da positron emission tomography, da Magnetic resonance cholangiopancreatography na iya zama da amfani a wasu lokuta. Duban dan tayi na ciki ba shi da mahimmanci kuma zai rasa ƙananan ciwace-ciwacen ƙwayoyi, amma zai iya gano ciwon daji da suka yada zuwa hanta da kuma gina ruwa a cikin rami na peritoneal ( ascites ). Ana iya amfani da shi don gwajin farko mai sauri da arha kafin wasu fasahohin.
Ana iya amfani da biopsy ta kyakkyawan buri na allura, sau da yawa ta hanyar duban dan tayi na endoscopic, inda babu tabbas game da ganewar asali, amma ba a yawan buƙatar ganewar asali na tarihi don cire ƙwayar cuta ta hanyar tiyata don ci gaba.
Gwajin aikin hanta na iya nuna haɗin sakamakon da ke nuni da toshewar bile ducts ( tasowar bilirubin da aka haɗa, γ-glutamyl transpeptidase da matakan alkaline phosphatase ). CA19-9 (carbohydrate antigen 19.9) alama ce ta ciwace-ciwacen ƙwayar cuta wanda ake yawan ɗaukaka shi a cikin ciwon daji na pancreatic. Duk da haka, ba shi da hankali da ƙayyadaddun ƙayyadaddun bayanai, ba kalla ba saboda 5% na mutane ba su da antigen Lewis (a) kuma ba za su iya samar da CA19-9 ba. Yana da hankali na 80% da ƙayyadaddun 73% a cikin gano adenocarcinoma na pancreatic, kuma ana amfani dashi don bin sanannun lokuta maimakon ganewar asali.
Histopathology
gyara sashe.jpg)
Mafi yawan nau'in ciwon daji na pancreatic (adenocarcinoma) yawanci ana siffanta shi ta matsakaicin matsakaici zuwa ƙarancin bambance-bambancen tsarin glandular akan jarrabawar ganima. Akwai yawanci babba desmoplasia ko samuwar fibrous stroma ko tsarin nama wanda ya ƙunshi nau'ikan nau'ikan tantanin halitta (ciki har da myofibroblasts, macrophages, lymphocytes da ƙwayoyin mast ) da kayan da aka ajiye (kamar nau'in collagen na I da hyaluronic acid ). Wannan yana haifar da ƙwayar ƙwayar ƙwayar ƙwayar ƙwayar ƙwayar ƙwayar ƙwayar ƙwayar ƙwayar ƙwayar ƙwayar ƙwayar ƙwayar ƙwayar ƙwayar jini (hypovascular) da haka na oxygen ( cututtuka hypoxia ). [50] Ana tsammanin hakan yana hana yawancin magungunan chemotherapy isa ga ciwace-ciwacen daji, a matsayin daya daga cikin abubuwan da ke sa cutar kansa ke da wuyar magancewa.
| Cancer type | Relative incidence[51] | Microscopy findings[51] | Micrograph | Immunohistochemistry markers[51] | Genetic alterations[51] |
|---|---|---|---|---|---|
| Pancreatic ductal adenocarcinoma (PDAC) | 90% | Glands and desmoplasia | 
|
||
| Pancreatic acinar cell carcinoma (ACC) | 1% to 2% | Granular appearance | 
|
||
| Adenosquamous carcinoma | 1% to 4%[52] | Combination of gland-like cells and squamous epithelial cells. | 
|
Positive for:
Negative for: |
|
| Pancreatic neuroendocrine tumor | 5% | Multiple nests of tumor cells |  |
||
| Pre-cancer below for comparison: | |||||
| Precancer: | 3% | Mucinous epithelial cells.[53] Growth within the pancreatic ducts.[54] | 
|
||
Tsayawa
gyara sasheExocrine cancers
gyara sasheCiwon daji na pancreatic yawanci ana yin shi ne bayan CT scan . Mafi yawan tsarin sarrafa kansar da ake amfani da shi don ciwon daji na pancreatic shine wanda Kwamitin Hadin gwiwar Ciwon daji na Amurka (AJCC) ya tsara tare da Union for International Cancer Control (UICC). Tsarin tsarawa na AJCC-UICC yana zayyana manyan matakai guda huɗu gabaɗaya, kama daga farkon zuwa cuta mai ci gaba, dangane da rarrabuwar TNM na girman T umor, yaɗa zuwa ƙwayoyin lymph N, da M etastasis. [55]
Don taimakawa yanke shawara a kan jiyya, kumburin zuwa rukuni uku dangane da ko cirewar an yanke hukunci don zama "singectable schoctable", ko "ba a kula da shi ba", ko "ba a kula da shi ba", ko kuma "ba a kula da shi ba", ko "ba a kula da shi ba", ko "ba mai sakewa ba". [56] Lokacin da cutar ta kasance a matakin farko (AJCC-UICC matakan I da II), ba tare da yaduwa zuwa manyan hanyoyin jini ko gabobin nesa kamar hanta ko huhu ba, ana iya yin tiyatar ƙwayar ƙwayar cuta ta al'ada, idan mai haƙuri ya yarda. don gudanar da wannan babban tiyata kuma ana tunanin ya dace sosai.
Tsarin tsari na AJCC-UICC yana ba da damar bambanci tsakanin ciwace-ciwacen mataki na III waɗanda aka yanke hukunci su zama "lalacewar iyaka" (inda aikin tiyata yana yiwuwa a zahiri saboda axis celiac da babban jijiya mesenteric har yanzu suna da 'yanci) da waɗanda suke "marasa tushe" (saboda ƙari). cututtuka masu tasowa a cikin gida); dangane da ƙarin cikakkun bayanai na TNM, waɗannan ƙungiyoyi biyu sun dace da T3 da T4 bi da bi.
_CRUK_179.svg)
- Pancreatic cancer staging (TNM classification)
-
 Stage T1 ciwon daji na pancreatic
Stage T1 ciwon daji na pancreatic -
 Stage T2 ciwon daji na pancreatic
Stage T2 ciwon daji na pancreatic -
 Stage T3 ciwon daji na pancreatic
Stage T3 ciwon daji na pancreatic -
 Stage T4 ciwon daji na pancreatic
Stage T4 ciwon daji na pancreatic -
 Ciwon daji na pancreatic a cikin nodes na lymph na kusa - Mataki na N1
Ciwon daji na pancreatic a cikin nodes na lymph na kusa - Mataki na N1




_CRUK_178.svg)
Ci gaban adenocarcinomas na gida sun bazu zuwa gabobin da ke makwabtaka da su, wanda zai iya zama kowane ɗayan waɗannan (a cikin ƙayyadaddun tsari na raguwa): duodenum, ciki, hanji mai jujjuyawa, saifa, glandar adrenal, ko koda . Sau da yawa suna yaduwa zuwa mahimman jini ko tasoshin lymphatic da jijiyoyi da ke tafiya kusa da pancreas, yana sa tiyata ya fi wuya. Shafukan yau da kullun don yaduwar metastatic (cututtukan mataki na IV) sune hanta, rami na peritoneal da huhu, duk waɗanda ke faruwa a cikin 50% ko fiye na ci gaba da ci gaba. [57]
PanNETs
gyara sasheRarraba 2010 WHO na ciwace-ciwacen daji na tsarin narkewar abinci ya ba dukkan ciwace-ciwacen ciwace-ciwacen ƙwayar cuta (PanNETs) zuwa nau'ika 2010 da WHO ta ware su daga "NET G1" zuwa "NET G3"). Cibiyar Ciwon Kankara ta Ƙasa ta Amurka ta ba da shawarar amfani da tsarin AJCC-UICC iri ɗaya kamar adenocarcinoma na pancreatic. [58] :52Yin amfani da wannan makirci, sakamakon mataki-mataki na PanNETs ya bambanta da na ciwon daji na exocrine. [59] Ƙungiyar Neuroendocrine Tumor Society ta Turai ta gabatar da wani tsarin TNM na daban don PanNETs.
Rigakafi da dubawa
gyara sasheBaya ga shan taba, Ƙungiyar Ciwon daji ta Amirka ta ba da shawarar kiyaye nauyin lafiya, da kuma ƙara yawan amfani da 'ya'yan itatuwa, kayan lambu, da dukan hatsi, yayin da rage yawan amfani da ja da nama mai sarrafa, ko da yake babu wata shaida mai mahimmanci wannan zai hana ko rage ciwon daji na pancreatic musamman. . [60] Binciken bincike na 2014 ya kammala cewa akwai shaidar cewa cin 'ya'yan itacen citrus da curcumin sun rage hadarin ciwon daji na pancreatic, yayin da akwai yiwuwar tasiri mai amfani daga dukan hatsi, folate, selenium, da kifi maras soyayyen.
A cikin yawan jama'a, ba a ɗaukar gwajin manyan ƙungiyoyi masu tasiri kuma yana iya zama cutarwa har zuwa 2019, [61] kodayake sabbin dabaru, da kuma tantance ƙungiyoyin da aka yi niyya, ana kimanta su.[62][63] Duk da haka, ana ba da shawarar yin gwaje-gwaje na yau da kullun tare da duban dan tayi na endoscopic da MRI / CT ga waɗanda ke da babban haɗari daga gadon gado.[64]
Gudanarwa
gyara sasheExocrine ciwon daji
gyara sasheMahimmin ƙima da aka yi bayan ganewar asali shine ko cirewar ƙwayar ƙwayar cuta zai yiwu (duba Staging ), saboda wannan shine kawai maganin wannan ciwon daji. Ko za a iya ba da aikin tiyata ko a'a ya dogara da yadda ciwon daji ya yadu. Matsakaicin wurin da ƙari yake shi ma muhimmin abu ne, kuma CT na iya nuna yadda yake da alaƙa da manyan hanyoyin jini da ke wucewa kusa da pancreas. Hakanan dole ne a tantance lafiyar mutum gaba ɗaya, kodayake shekarun kansa ba shi ne cikas ga tiyata ba.
Chemotherapy da, a ɗan ƙarami, ana iya ba da maganin rediyo ga yawancin mutane, ko tiyata yana yiwuwa ko a'a. Kwararrun masana sun ba da shawarar cewa kula da ciwon daji na pancreatic ya kamata ya kasance a hannun ƙungiyoyi masu yawa ciki har da ƙwararrun masana a fannoni da yawa na oncology, kuma, saboda haka, mafi kyawun gudanar da shi a cikin manyan cibiyoyin.
Manazarta
gyara sashe- ↑ "What is Cancer? Defining Cancer". National Cancer Institute, National Institutes of Health. 7 March 2014. Archived from the original on 25 June 2014. Retrieved 5 December 2014.
- ↑ 2.00 2.01 2.02 2.03 2.04 2.05 2.06 2.07 2.08 2.09 2.10 2.11 2.12 2.13 World Cancer Report. World Health Organization. 2014. Chapter 5.7. ISBN 978-92-832-0429-9.
- ↑ 3.0 3.1 Unless otherwise specified in boxes, reference is: Pishvaian MJ, Brody JR (March 2017). "Therapeutic Implications of Molecular Subtyping for Pancreatic Cancer". Oncology. 31 (3): 159–66, 168. PMID 28299752.
- ↑ 4.0 4.1 4.2 4.3 4.4 "Pancreatic Cancer Treatment (PDQ®) Patient Version". National Cancer Institute. National Institutes of Health. 17 April 2014. Archived from the original on 5 July 2014. Retrieved 8 June 2014.
- ↑ 5.00 5.01 5.02 5.03 5.04 5.05 5.06 5.07 5.08 5.09 5.10 5.11 5.12 5.13 5.14 Ryan DP, Hong TS, Bardeesy N (September 2014). "Pancreatic adenocarcinoma". The New England Journal of Medicine. 371 (11): 1039–49. doi:10.1056/NEJMra1404198. PMID 25207767.
- ↑ 6.00 6.01 6.02 6.03 6.04 6.05 6.06 6.07 6.08 6.09 6.10 Bond-Smith G, Banga N, Hammond TM, Imber CJ (May 2012). "Pancreatic adenocarcinoma". BMJ. 344 (may16 1): e2476. doi:10.1136/bmj.e2476. PMID 22592847. S2CID 206894869.
- ↑ 7.00 7.01 7.02 7.03 7.04 7.05 7.06 7.07 7.08 7.09 7.10 7.11 7.12 7.13 7.14 7.15 7.16 7.17 Wolfgang CL, Herman JM, Laheru DA, Klein AP, Erdek MA, Fishman EK, Hruban RH (September 2013). "Recent progress in pancreatic cancer". CA: A Cancer Journal for Clinicians. 63 (5): 318–48. doi:10.3322/caac.21190. PMC 3769458. PMID 23856911.
- ↑ 8.0 8.1 8.2 8.3 Vincent A, Herman J, Schulick R, Hruban RH, Goggins M (August 2011). "Pancreatic cancer" (PDF). Lancet. 378 (9791): 607–20. doi:10.1016/S0140-6736(10)62307-0. PMC 3062508. PMID 21620466. Archived from the original (PDF) on 12 January 2015.
- ↑ "Draft Recommendation Statement: Pancreatic Cancer: Screening – US Preventive Services Task Force". www.uspreventiveservicestaskforce.org. Retrieved 11 February 2019.
- ↑ "Can pancreatic cancer be prevented?". American Cancer Society. 11 June 2014. Archived from the original on 13 November 2014. Retrieved 13 November 2014.
- ↑ Bardou M, Le Ray I (December 2013). "Treatment of pancreatic cancer: A narrative review of cost-effectiveness studies". Best Practice & Research. Clinical Gastroenterology. 27 (6): 881–92. doi:10.1016/j.bpg.2013.09.006. PMID 24182608.
- ↑ Wang H, Naghavi M, Allen C, Barber RM, Bhutta ZA, Carter A, et al. (GBD 2015 Mortality and Causes of Death Collaborators) (October 2016). "Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet. 388 (10053): 1459–1544. doi:10.1016/s0140-6736(16)31012-1. PMC 5388903. PMID 27733281.
- ↑ "Cancer facts and figures – Why we exist – Pancreatic Cancer Research Fund". www.pcrf.org.uk. Retrieved 5 April 2019.
- ↑ "Pancreatic Cancer – Cancer Stat Facts". SEER (in Turanci). Retrieved 4 April 2019.
- ↑ "Cancer Facts & Figures 2010" (PDF). American Cancer Society. 2010. Archived from the original (PDF) on 14 January 2015. Retrieved 5 December 2014. See p. 4 for incidence estimates, and p. 19 for survival percentages.
- ↑ "Pancreatic Cancer Treatment (PDQ®) Health Professional Version". National Cancer Institute. National Institutes of Health. 21 February 2014. Archived from the original on 22 October 2014. Retrieved 24 November 2014. "The highest cure rate occurs if the tumor is truly localized to the pancreas; however, this stage of disease accounts for less than 20% of cases. In cases with localized disease and small cancers (<2 cm) with no lymph-node metastases and no extension beyond the capsule of the pancreas, complete surgical resection is still associated with a low actuarial five-year survival rate of 18% to 24%."
- ↑ Harris RE (2013). "Epidemiology of pancreatic cancer". Epidemiology of Chronic Disease. Jones & Bartlett. pp. 181–190. ISBN 978-0-7637-8047-0. Archived from the original on 24 June 2016.
- ↑ Öberg K, Knigge U, Kwekkeboom D, Perren A, et al. (ESMO Guidelines Working Group) (October 2012). "Neuroendocrine gastro-entero-pancreatic tumors: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up". Annals of Oncology. 23 Suppl 7 (suppl 7): vii124-30. doi:10.1093/annonc/mds295. PMID 22997445. (Table 5 outlines the proposed TNM staging system for PanNETs.)
- ↑ Handbook of Pancreatic Cancer. New York: Springer. 2009. p. 288. ISBN 978-0-387-77497-8. Archived from the original on 10 September 2017. Retrieved 12 June 2016.
- ↑ 20.0 20.1 Govindan R (2011). DeVita, Hellman, and Rosenberg's Cancer: Cancer: Principles & Practice of Oncology (9th ed.). Lippincott Williams & Wilkins. Chapter 35: Cancer of the Pancreas: Surgical Management. ISBN 978-1-4511-0545-2. Online edition, with updates to 2014
- ↑ 21.0 21.1 Tobias JS, Hochhauser D (2014). Cancer and its Management (7th ed.). p. 297. ISBN 978-1-118-46871-5.
- ↑ Farrell JJ, Fernández-del Castillo C (June 2013). "Pancreatic cystic neoplasms: management and unanswered questions". Gastroenterology. 144 (6): 1303–15. doi:10.1053/j.gastro.2013.01.073. PMID 23622140.
- ↑ 23.0 23.1 The PanNET denomination is in line with WHO guidelines for the classification of tumors of the digestive system "WHO classification of tumours of the digestive system – NLM Catalog – NCBI". Archived from the original on 9 September 2017. Retrieved 7 September 2017. published in 2010. Historically, PanNETs have also been referred to by a variety of terms, and are still commonly called "pancreatic endocrine tumors". See: Klimstra DS, Modlin IR, Coppola D, Lloyd RV, Suster S (August 2010). "The pathologic classification of neuroendocrine tumors: a review of nomenclature, grading, and staging systems". Pancreas. 39 (6): 707–12. doi:10.1097/MPA.0b013e3181ec124e. PMID 20664470. S2CID 3735444.
- ↑ 24.0 24.1 24.2 Burns WR, Edil BH (March 2012). "Neuroendocrine pancreatic tumors: guidelines for management and update". Current Treatment Options in Oncology. 13 (1): 24–34. doi:10.1007/s11864-011-0172-2. PMID 22198808. S2CID 7329783.
- ↑ The Medical Subject Headings indexing system refers to "islet cell carcinoma", which is subdivided into gastrinoma, glucagonoma, somatostatinoma, and VIPoma. See: 2014 MeSH tree at "Pancreatic Neoplasms [C04.588.322.475]" Archived 19 ga Maris, 2016 at the Wayback Machine 16 October 2014
- ↑ "Islet Cell Tumors of the Pancreas / Endocrine Neoplasms of the Pancreas". The Sol Goldman Pancreas Cancer Research Center. Johns Hopkins Medicine. 2012. Archived from the original on 5 January 2015. Retrieved 5 January 2015.
- ↑ Cite error: Invalid
<ref>tag; no text was provided for refs namedTobias - ↑ De La Cruz MS, Young AP, Ruffin MT (April 2014). "Diagnosis and management of pancreatic cancer". American Family Physician. 89 (8): 626–32. PMID 24784121.
- ↑ 29.0 29.1 Alberts SR, Goldberg RM (2009). "Chapter 9: Gastrointestinal tract cancers". In Casciato DA, Territo MC (eds.). Manual of clinical oncology. Lippincott Williams & Wilkins. pp. 188–236. ISBN 978-0-7817-6884-9.
- ↑ Pannala R, Basu A, Petersen GM, Chari ST (January 2009). "New-onset diabetes: a potential clue to the early diagnosis of pancreatic cancer". The Lancet. Oncology. 10 (1): 88–95. doi:10.1016/S1470-2045(08)70337-1. PMC 2795483. PMID 19111249.
- ↑ "Chapter 15; Pancreas" (PDF). Manual for Staging of Cancer (2nd ed.). American Joint Committee on Cancer. pp. 95–98. Archived (PDF) from the original on 29 November 2014. See p. 95 for citation regarding "... lesser degree of involvement of bones and brain and other anatomical sites."
- ↑ Sperti C, Moletta L, Patanè G (October 2014). "Metastatic tumors to the pancreas: The role of surgery". World Journal of Gastrointestinal Oncology. 6 (10): 381–92. doi:10.4251/wjgo.v6.i10.381. PMC 4197429. PMID 25320654.
- ↑ "Causes of pancreatic cancer". NHS Choices. National Health Service, England. 7 October 2014. Archived from the original on 6 November 2014. Retrieved 5 December 2014.
- ↑ Anderson, Laura N.; Cotterchio, Michelle; Gallinger, Steven (5 February 2009). "Lifestyle, dietary, and medical history factors associated with pancreatic cancer risk in Ontario, Canada". Cancer Causes & Control. 20 (6): 825–34. doi:10.1007/s10552-009-9303-5. ISSN 0957-5243. PMC 3907069. PMID 19194662.
- ↑ Bosetti C, Lucenteforte E, Silverman DT, Petersen G, Bracci PM, Ji BT, et al. (July 2012). "Cigarette smoking and pancreatic cancer: an analysis from the International Pancreatic Cancer Case-Control Consortium (Panc4)". Annals of Oncology. 23 (7): 1880–88. doi:10.1093/annonc/mdr541. PMC 3387822. PMID 22104574.
- ↑ De Rubeis, Vanessa; Cotterchio, Michelle; Smith, Brendan T.; Griffith, Lauren E.; Borgida, Ayelet; Gallinger, Steven; Cleary, Sean; Anderson, Laura N. (1 September 2019). "Trajectories of body mass index, from adolescence to older adulthood, and pancreatic cancer risk; a population-based case–control study in Ontario, Canada". Cancer Causes & Control (in Turanci). 30 (9): 955–66. doi:10.1007/s10552-019-01197-9. ISSN 1573-7225. PMC 6685923. PMID 31230151.
- ↑ De Rubeis, Vanessa; Cotterchio, Michelle; Smith, Brendan T.; Griffith, Lauren E.; Borgida, Ayelet; Gallinger, Steven; Cleary, Sean; Anderson, Laura N. (1 September 2019). "Trajectories of body mass index, from adolescence to older adulthood, and pancreatic cancer risk; a population-based case–control study in Ontario, Canada". Cancer Causes & Control (in Turanci). 30 (9): 955–66. doi:10.1007/s10552-019-01197-9. ISSN 1573-7225. PMC 6685923. PMID 31230151.
- ↑ 38.0 38.1 Reznik R, Hendifar AE, Tuli R (2014). "Genetic determinants and potential therapeutic targets for pancreatic adenocarcinoma". Frontiers in Physiology. 5: 87. doi:10.3389/fphys.2014.00087. PMC 3939680. PMID 24624093.
- ↑ Greenhalf W, Grocock C, Harcus M, Neoptolemos J (May 2009). "Screening of high-risk families for pancreatic cancer". Pancreatology. 9 (3): 215–22. doi:10.1159/000210262. PMID 19349734. S2CID 29100310.
- ↑ Venturi, Sebastiano (January 2021). "Cesium in Biology, Pancreatic Cancer, and Controversy in High and Low Radiation Exposure Damage—Scientific, Environmental, Geopolitical, and Economic Aspects". International Journal of Environmental Research and Public Health (in Turanci). 18 (17): 8934. doi:10.3390/ijerph18178934. PMC 8431133 Check
|pmc=value (help). PMID 34501532 Check|pmid=value (help). Text was copied from this source, which is available under a Creative Commons Attribution 4.0 International License.
Text was copied from this source, which is available under a Creative Commons Attribution 4.0 International License.
- ↑ 41.0 41.1 "Cancer Facts and Figures 2014" (PDF). American Cancer Society. Archived (PDF) from the original on 18 December 2014. Retrieved 5 January 2015., p. 19, "Though evidence is still accumulating, consumption of red or processed meat, or meat cooked at very high temperatures, may slightly increase risk."
- ↑ Larsson SC, Wolk A (January 2012). "Red and processed meat consumption and risk of pancreatic cancer: meta-analysis of prospective studies". British Journal of Cancer. 106 (3): 603–07. doi:10.1038/bjc.2011.585. PMC 3273353. PMID 22240790.
- ↑ Pericleous M, Rossi RE, Mandair D, Whyand T, Caplin ME (January 2014). "Nutrition and pancreatic cancer". Anticancer Research. 34 (1): 9–21. PMID 24403441.
- ↑ Delpu Y, Hanoun N, Lulka H, Sicard F, Selves J, Buscail L, et al. (March 2011). "Genetic and epigenetic alterations in pancreatic carcinogenesis". Current Genomics. 12 (1): 15–24. doi:10.2174/138920211794520132. PMC 3129039. PMID 21886451.
- ↑ Rooney SL, Shi J (October 2016). "Intraductal Tubulopapillary Neoplasm of the Pancreas: An Update From a Pathologist's Perspective". Archives of Pathology & Laboratory Medicine. 140 (10): 1068–73. doi:10.5858/arpa.2016-0207-RA. PMID 27684978.
- ↑ "The human pathology proteome in pancreatic cancer – The Human Protein Atlas". www.proteinatlas.org. Archived from the original on 3 July 2020. Retrieved 28 September 2017.
- ↑ Uhlen M, Zhang C, Lee S, Sjöstedt E, Fagerberg L, Bidkhori G, et al. (August 2017). "A pathology atlas of the human cancer transcriptome". Science. 357 (6352): eaan2507. doi:10.1126/science.aan2507. PMID 28818916.
- ↑ Lewis MA, Yao JC (February 2014). "Molecular pathology and genetics of gastrointestinal neuroendocrine tumours". Current Opinion in Endocrinology, Diabetes and Obesity. 21 (1): 22–27. doi:10.1097/MED.0000000000000033. PMID 24310147. S2CID 31094880.
- ↑ Thakker RV, Newey PJ, Walls GV, Bilezikian J, Dralle H, Ebeling PR, et al. (September 2012). "Clinical practice guidelines for multiple endocrine neoplasia type 1 (MEN1)". The Journal of Clinical Endocrinology and Metabolism. 97 (9): 2990–3011. doi:10.1210/jc.2012-1230. PMID 22723327.
- ↑ Empty citation (help)
- ↑ 51.0 51.1 51.2 51.3 Unless otherwise specified in boxes, reference is: Pishvaian MJ, Brody JR (March 2017). "Therapeutic Implications of Molecular Subtyping for Pancreatic Cancer". Oncology. 31 (3): 159–66, 168. PMID 28299752.
- ↑ Skafida E, Grammatoglou X, Glava C, Zissis D, Paschalidis N, Katsamagkou E, et al. (February 2010). "Adenosquamous carcinoma of the pancreas: a case report". Cases Journal. 3 (1): 41. doi:10.1186/1757-1626-3-41. PMC 2825199. PMID 20205828.
- ↑ Diana Agostini-Vulaj. "Pancreas – Exocrine tumors / carcinomas – Intraductal papillary mucinous neoplasm (IPMN)". Pathology Outlines. Topic Completed: 1 July 2018. Revised: 9 March 2020
- ↑ Adsay V, Mino-Kenudson M, Furukawa T, Basturk O, Zamboni G, Marchegiani G, et al. (January 2016). "Pathologic Evaluation and Reporting of Intraductal Papillary Mucinous Neoplasms of the Pancreas and Other Tumoral Intraepithelial Neoplasms of Pancreatobiliary Tract: Recommendations of Verona Consensus Meeting". Annals of Surgery. 263 (1): 162–77. doi:10.1097/SLA.0000000000001173. PMC 4568174. PMID 25775066.
- ↑ Cascinu S, Falconi M, Valentini V, Jelic S (May 2010). "Pancreatic cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up". Annals of Oncology. 21 Suppl 5 (Supplement 5): v55–58. doi:10.1093/annonc/mdq165. PMID 20555103.
- ↑ Empty citation (help)
- ↑ Zyromski NJ, Nakeeb A, Lillemoe KD (2010). Silberman H, Silberman AW (eds.). Principles and practice of surgical oncology : multidisciplinary approach to difficult problems (online ed.). Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins. Chapter 35. ISBN 978-0-7817-6546-6. Archived from the original on 6 February 2015. Retrieved 3 November 2014.
- ↑ "Neuroendocrine tumors, NCCN Guidelines Version 1.2015" (PDF). National Comprehensive Cancer Network, Inc. NCCN). 11 November 2014. Retrieved 25 December 2014.
- ↑ National Cancer Institute. Pancreatic Neuroendocrine Tumors (Islet Cell Tumors) Treatment (PDQ®) Incidence and Mortality "Pancreatic Neuroendocrine Tumors (Islet Cell Tumors) Treatment (PDQ®)–Health Professional Version". Archived from the original on 4 January 2015. Retrieved 29 December 2014.
- ↑ "Diet and activity factors that affect risks for certain cancers: Pancreatic cancer section". American Cancer Society. 20 August 2012. Archived from the original on 4 November 2014. Retrieved 4 November 2014.
- ↑ Owens DK, Davidson KW, Krist AH, Barry MJ, Cabana M, Caughey AB, et al. (August 2019). "Screening for Pancreatic Cancer: US Preventive Services Task Force Reaffirmation Recommendation Statement". JAMA. 322 (5): 438–44. doi:10.1001/jama.2019.10232. PMID 31386141.
- ↑ He XY, Yuan YZ (August 2014). "Advances in pancreatic cancer research: moving towards early detection". World Journal of Gastroenterology. 20 (32): 11241–48. doi:10.3748/wjg.v20.i32.11241. PMC 4145762. PMID 25170208.
- ↑ Okano K, Suzuki Y (August 2014). "Strategies for early detection of resectable pancreatic cancer". World Journal of Gastroenterology. 20 (32): 11230–40. doi:10.3748/wjg.v20.i32.11230. PMC 4145761. PMID 25170207.
- ↑ Goggins M, Overbeek KA, Brand R, Syngal S, Del Chiaro M, Bartsch DK, et al. (January 2020). "Management of patients with increased risk for familial pancreatic cancer: updated recommendations from the International Cancer of the Pancreas Screening (CAPS) Consortium". Gut. 69 (1): 7–17. doi:10.1136/gutjnl-2019-319352. PMC 7295005. PMID 31672839.